
My friend is suffering with shingles in her ear of all places . Poor woman now has bells palsey , shes been taken into hospital . She was healthy and well and ate a very healthy diet . How on earth she caught the virus we dont know . Is it air born or caught from someone ?
She must have had chicken pox as a child. For whatever reason the virus has reactivated. I hope your friend feels better soon. It’s dangerously close to the brain so I hope her GP is monitoring the situation.
1 Like
She had chicken pox as a child and the virus stayed dormant in her system for years and then reactivated as shingles.
1 Like
I had the shingles jab a few years ago. People between 70/80 are eligible, it’s on the NHS & free. I have never had shingles but I had chickenpox as a child.
Im too scared to have the shingles jab in case it makes me sick . A couple of friends have actually got shingles days after and been very poorly
Which shingles vaccine do you have in UK?
Here in Australia it used to be Zostavax which is a live vaccine, so that is possible. Rare but possible and because of that couldn’t be given to immunocompromised people.
As of Nov1st last year zostavax was superseded by Shingrix which is not a live vaccine and so cannot do that and can be given to everyone
1 Like
We are moving over to the non-live Shingrix vaccine in U.K., starting last Autumn here too. Before that I think it was generally reserved for people with weakened immune systems.
I sensed there was some reluctance to offer it to everyone but I’m not sure why - is it a more expensive vaccine?
However, like all the changes in age eligibility for the Shingles vaccine, the changes seem to be complicated because now, which vaccine you receive not only depends on whether you are immuno-compromised or not but also seems to be age-dependent too.
I don’t know why they have added in this extra complication of saying people already aged 70-79 may be offered either of the two vaccines but people who reach the eligible age of 65 or 70 in future will be offered only Shingrix - maybe it is worded this way to allow them use up any old stocks of Zostovax vaccines and will switch over completely when all old Stocks have been used up?
Unless in your experience with vaccines, you can see another reason?
From the Gov announcement made last year:
The vaccine that is used in the programme is also changing. All newly eligible individuals will be offered two doses of the non-live vaccine Shingrix instead of the live vaccine Zostavax.
From 1 September 2023:
• Those aged 70-79 will still be able to get the shingles vaccine from their GP practice.
They will either be offered one dose of Zostavax or two doses of Shingrix (6 to 12
months apart)
• All those aged 50 and over with a weakened immune system will be offered two doses
of the Shingrix vaccine by their GP practice (8 weeks to 6 months apart).
• Those turning 65 and 70 will be offered two doses of the Shingrix vaccine (6 to 12
months apart) by their GP practice as they become eligible (eligibility will go down to 60 years old from 2028)
just checked the NHS site and it is both here
perhaps people have a choice if they ask their GP
so it would seem :
1 Like
You should tell your GP you want the Shingrix vaccine or nothing. They should hopefully agree it’s better to give you Shingrix than leave you unprotected.
Thanks for that info @AnnieS
Yep - that answers my question!
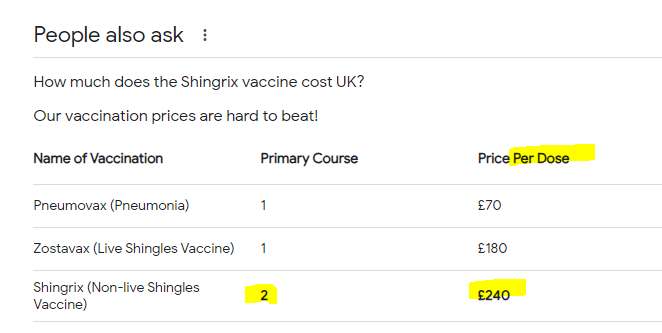
I presume the prices on the list you posted is the “retail price” for a private vaccination.
Since I posted my last comment, I did find an NHS document, giving advice to GP Surgeries about the new implementation schedule - it mentioned in there they should use up any existing Zostovax stocks so they are not wasted but not order any more when stocks run out.
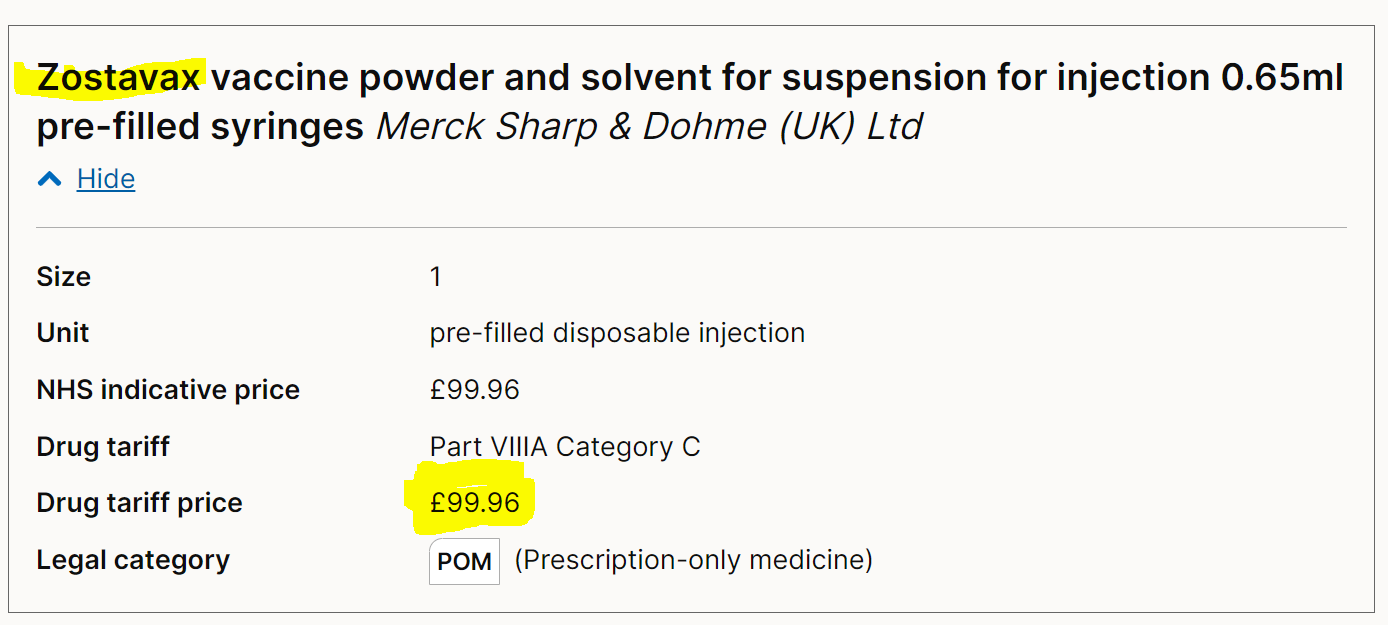
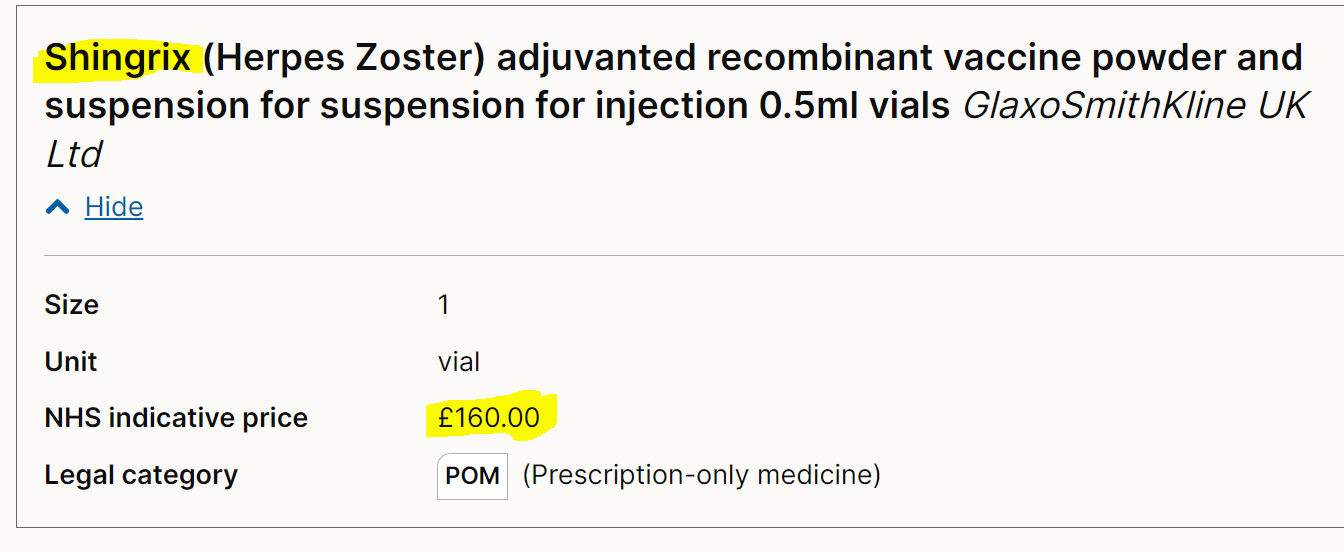
They also cautioned against over-ordering / overstocking supplies of Shingrix because it was so expensive - they quoted a cost price that NHS have to pay for the vaccines as £99.96 per dose for Zostovax and £160 per dose for Shingrix - so the vaccine cost per patient vaccinated is £320 instead of £100 and the programme is being extended to a wider age group.
Looking at the vaccination prices you found, it ties in with those price differences.
It also shows that the private vaccination fees are not such a “rip off” as I first thought when I was considering having Shingrix vaccination privately rather than wait until I’m 70 for a free one - if at least £160 of that £240 for each dose is to cover the cost of the vaccine, then the private company must be charging no more than £80 per vaccination to cover their staff costs and other overheads and make some profit.
sorry I meant to post this
Also important to note that you need 2 of the Shingrix vaccines so that £320 in total plus the administration charge.
Interesting.
I am always interested in comparisons of schedules etc from country to country.
Here in Australia, Zostavax has been completely superseded by Shingrix.
( am not sure if Zostavax still available on private script if people want to pay cheaper - and don’t qualify for either on the NIP - national immunisation program - ie govt funded)
But NIP providers (such as where I work) were told to discard Zostavax stocks once Shingrix was available
As I was over 50 but under 65 - therefore qualified by age for private script Zostavax but not yet for govt funded Shingrix - I took the liberty of giving myself a free Zostavax, since it was going to be discarded anyway.
I’m sure other places did likewise.
Zostavax was NIP funded for people between 70 - 80 only (but not if immunocompromised) but available on private script for anyone over 50
Shingrix is available for anyone over 65, Aboriginal people over 50 and people over 18 with certain severe immunocompromise issues. (eg transplant reciprients, haematoligical malignancies)
ETA - if people had NIP funded Zostavax, they can still have Shingrix - but not until 5 years later)
2 Likes
I’ve just checked and Zostavax is being abandoned because protection wanes significantly over the longer term.
1 Like
And the fact it is a live vaccine which Shingrix is not, therefore can be given to everyone, immunocompromised or not.
you got that?
I think the confusion arises because chickenpox is contagious in the air while shingles by touch
Shingles is not contagious. But if someone comes into contact with the rash at a certain stage, they may contract the varicella-zoster virus and develop chickenpox. If they have chickenpox, shingles can develop later in life. To prevent transmitting the virus, keep shingles rashes covered.
1 Like
I am a vaccination nurse of 40 years. Shingles are not contagious. It is an autoimmune disease, which means that your body’s own cells attack themselves - why, nobody knows.
It usually develops on the lower / upper back, travels round to the side and then round to the abdomen, but not always. There are atypical shingles.
It’s horrendously painful, and many people have to be admitted to hospital on opioid medication. Sometimes, these do not help though.
Shingles derives from a virus that lies dormant on nerve cells, after contracting chicken pox. It gets activated from factors like stress, smoking, drinking too much, being run down, sick and other factors.
Shingles returns to Mrs mart from time to time.
1 Like